The diagnosis: there’s something terribly wrong with me. But we all suspected that a long time ago. HAHA GOOD JOKE KENNETT.
I just found out that I have hypothyroidism. It explains a lot. Don’t worry, it’s not contagious. It can’t be spread by a cough or anal. It’s genetic, just like herpes. Read along to find out what it is, why you should send me a get well soon care package filled with chocolate and smoked herring, and how the rest of my life will be ruined now that I have a disability other than being a white, upper-middle-class male of above average height.

“How to remain incredibly calm while being choked out”
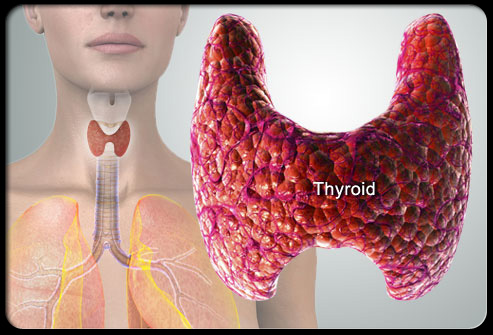
As the first image shows, your thyroid is a gland in your throat that has one purpose: to secrete thyroid hormones. Thyroid hormones (the main ones being T3 and T4) control your basal metabolic rate, bone growth (in children), protein synthesis, metabolism of fat, carbohydrates, and protein, and how your body uses and reacts to other hormones. Basically, it does a lot of important shit. Mine, however, has fallen asleep on the job. Permanently.
Science talk
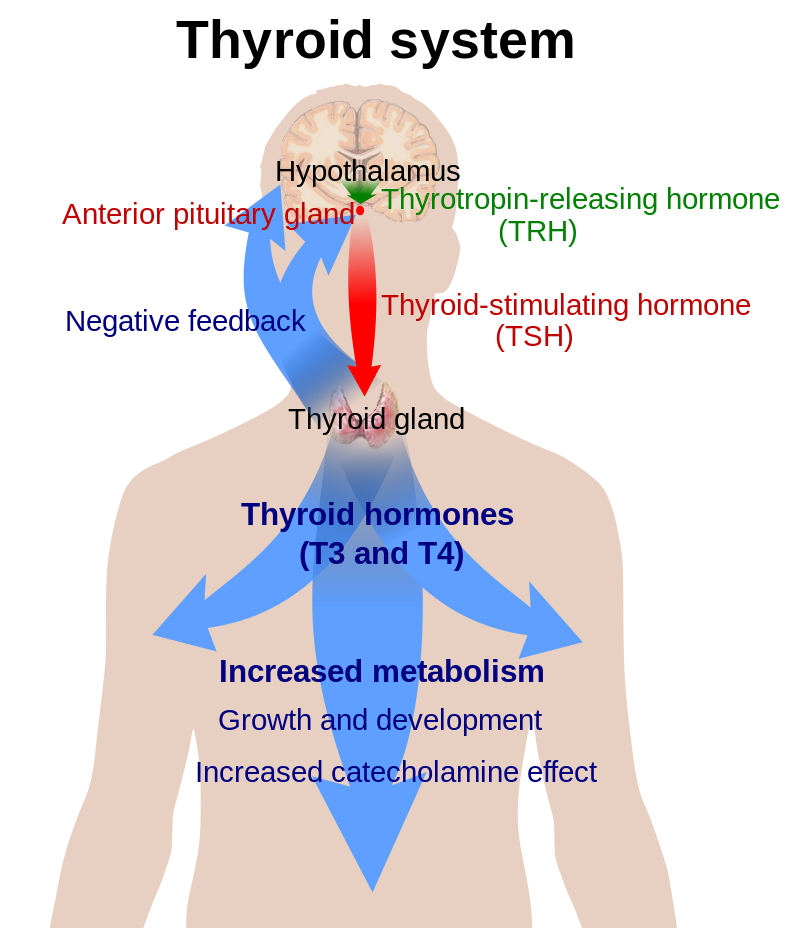
The hypothalamus, located up in your head, is the first in the chain of command when it comes to your endocrine system (hormones and stuff). When hormones need making, your hypothalamus gets called up and, like any good manager, delegates the work to other body parts–first the pituitary gland. Don’t bag on the hypothalamus too much. It’s got other, more important stuff to do anyways.
So, the hypothalamus releases TRH (thyrotropin-releasing hormone), which lets the pituitary know that it should start making TSH (thyroid-stimulating hormone). TSH tells the thyroid gland to start pumping out thyroid hormone, which as I described above, tells the rest of your body how to use energy. There’s a lot of middle management in the endocrine system, which is why I believe there are so many problems with it.
Wikipedia, you so smart. Thanks for making me smart to.
Anywho, my thyroid no longer works. It might be that it’s been out of order for a long, long time. According to my doctor, my thyroid is essentially useless and has “shut down.” I discovered this when, a few weeks ago, I went in to get a prescription for sleeping meds. I’ve been having a lot of trouble sleeping lately, especially the past three or four months. My insomnia goes back at least a year but had been getting unbearable more recently.
The doctor decided to test my thyroid, with the initial inkling that it might be producing too much thyroid hormone, called hyperthyroidism with an E, which can lead to difficulty sleeping and an overly active metabolism. I ended up having hypothyroidism with an Ohhh–the opposite problem, but it can also impair sleep.
To test your thyroid function, they suck out some blood and count how much T3, T4, and TSH is in it. TSH, as you may recall, acts as a signal for your thyroid gland to produce thyroid hormones. So the higher your TSH, the more thyroid hormones your body craves. The lower your TSH, the less thyroid it craves. The normal TSH range for a healthy person is 0.5 to 5 microunits per milliliter. With a TSH of 5 to 10, you’re considered to have subclinical hypothyroidism, which means you probably don’t need to be medicated unless you’re experiencing a lot of the symptoms of hypothyroidism, which I’ll get into in just a second. If your TSH is over 10, you have overt hypothyroidism, meaning you should definitely consider getting treatment since your thyroid is currently on a downward spiral to hell. If left untreated over the years, subclinical hypothyroidism may eventually become overt, and once it’s overt it’s likely that it will eventually shut down altogether. I think. Remember, I’m not a doctor so you should definitely take everything I say as fact.
My TSH was “greater than” 150. One hundred and fifty. What the fuck. Apparently that particular lab’s test only goes to 150, meaning I was off the charts. My doctor tested me again just to be sure, and the second test came back the same.
Hypothyroidism is usually due to Hashimoto’s disease, which is a genetic disorder. Something like 90% of people with overt hypothyroidism have Hashimoto’s. As an autoimmune disease, Hashimoto’s confuses your body into attacking the thyroid gland until it’s dead. You can also have hypothyroidism if you’ve had thyroid surgery, thyroid cancer, not enough iodine in your diet, an inability to absorb iodine, or a few other equally rare scenarios. In my case, it’s Hashimoto’s, as I later had it tested and came back positive with a crap load of thyroid antibodies.
Symptoms
There are a lot of them. The blue ones are ones that I’ve noticed.
Fatigue
Muscle weakness
Inability to focus
Carpel Tunnel Syndrom
Decreased libido
Hearing loss
Dry skin
Hair loss/dry hair
Depression
Trouble falling asleep and staying asleep
Night sweats or hot flashes during sleep
Slow heart rate (mine is 28)
Weight gain
Trouble losing weight
Constipation
Irritability
Intolerance to the cold
Memory loss
Abnormal menstrual cycles (hypothyroidism is much more likely to strike women than men by the way)
Muscle cramps and aches
And even more. Basically it fucks you right up.
As you read through this list, you can see how I never thought anything was wrong with me, since these are all basically symptoms of training hard.
How did this happen?
You can’t get Hashimoto’s without a genetic predisposition, which only a small percentage of the population has to worry about. 3.5% of the population has Hashimoto’s (and 5% of the population has hypothyroidism), with women being 8-10 times more likely to develop it than men. It’s also very rare in young people, with post-menopausal women being the main victims. So why do I have it?
There is a hypothesis that if you’re genetically predisposed to Hashimoto’s (my mom and grandmother have it too), hard endurance training or stress may bring it on earlier in life. So I got it when I was in my 20s instead of my 50s due to hard training, or so the thinking goes. This has not been proven. Another way you can give yourself hypothyroidism is by taking a lot of testosterone or HGH.
Which brings me to the next chapter…
Doping
There is a growing number of elite runners that apparently have hypothyroidism. Galen Rupp is on that list, along with a bunch of other Nike runners. You may have come across this Wall Street Journal article that describes the unconventional approach that a certain doctor by the name of Jeff Brown uses when it comes to diagnosing elite athletes with hypothyroidism. Read: “doping doctor.”
At the time of the above article’s publication, Alberto Salazar had coached 30 elite Nike athletes, and 17% of those had been diagnosed with hypothyroidism by Dr. Brown. As you may recall, only 5% of the population actually has hypothyroidism, and most of those people are older women, not young males, and many of them do not need to be medicated as they do not have overt hypothyroidism. My theory is that Brown is replacing thyroid that was originally lost due to testosterone and HGH doping (testosterone and HGH both stunt the thyroid’s output). That, or there may be a small advantage for a healthy, non-hypothyroid person to microdose with synthetic thyroid. This is debatable, as google will tell you. In his rational, Dr. Brown believes that a TSH of 2.0 or higher requires medication. He is virtually alone in the medical world when it comes to this standard. Remember, 0.5 to 5 is considered healthy. My TSH is +150 and I’m still kicking, so I find it very hard to believe that someone with a value of 2.0 needs meds.
Note: synthetic thyroid isn’t even on WADA’s banned substance list since it hasn’t actually been shown to be a performance enhancer. That’s the part that leads me to question if Brown is covering up as well as fixing some of the health problems caused by HGH and testosterone doping.
So how do I deal with it?
Thank you baby jesus for the pharmaceutical industry and America, the land where taking a pill solves all your problems. As long as you have money for insurance. And your problems consist of restless leg syndrome and ED.
I have to take a pill every morning for the rest of my life called levothyroxine, which is synthetic thyroid. It’s the thyroid hormone T4, which the body converts to T3. It takes a few weeks to start kicking in, then a few months to dial in the correct dose. I’ll have to have my TSH values monitored two to three times a year for the rest of my life as well, to ensure I’m continuing to get the right dose. Taking too little levothyroxine will leave me fatigued and depressed. Too much and apparently it’ll be like I’m on crack, without any of the good side effects.
Training as an elite athlete who has hypothyroidism, even while medicated, is supposedly much more difficult than a healthy person’s training. I found some great info about hypothyroidism and endurance athletes from the smart words of world-renown running coach Steve Magness. Check out his website for the goods. His book The Science of Running is incredibly good too. Even if you’re just a cyclist you should still read it.
Anyways, as a runner who has had hypothyroidism since he was 14, Magness, claims that training is made extra difficult by this disease. One day you’re up, the next you’re down. There’s little consistency and it sometimes takes a lot longer to recover from hard workouts than it would for a normal athlete. Looking back, I’ve noticed this.
Since the hypothyroid sufferer’s body doesn’t get a natural, steady flow of thyroid hormones when it needs it, recovery becomes significantly impaired. I’ll take a pill every morning, but I won’t get that steady drip like a regular person, telling the body how to respond minute by minute throughout the day as it encounters stress and physical exertion.
But I’m optimistic. I think that this diagnosis means that I’ll be able to get back to where I was in 2013, and maybe even better. I’ve most likely had this going on for years now, since it’s a disease that develops over a long period of time. If I had to put a date on it, looking back I’d say that I really started noticing that something was a bit off in 2007. I had trained really hard that winter and could never kick the fatigue that came with it. I ended up taking most of the year off to recover, summing it up as just some severe overtraining. While I don’t doubt that I was severely overtrained, I think a part of the reason I wasn’t able to recover was due to my messed up thyroid.
While I continued getting stronger over the years, I’ve always struggled with going too hard and not being able to recover. One week I’d be great in training, then the following week I’d be dead by day two, even on the off chance when I decided to take adequate rest. I’d be shit for two months for some reason and then magically be fast again. This is a natural occurrence for any athlete, especially in a sport like cycling where the season is so long and the training and racing are so stressful. Again, that adds to the difficulty of self-diagnosis.
Things really didn’t start going downhill until 2014, which is when I believe my thyroid might have shit the bed altogether. After a really good season in 2013, I signed for a crappy little pro Swedish team that went belly up part way into 2014. I came home to the States half a year early and really depressed since my dream had been shattered, and I could never get my legs going again that year. I’m wiling to bet that a large part of that lingering depression and lack of fitness was due to my good for nothing thyroid, not just the team folding.
Then in the fall of 2014 my wife Adelaide was out training for an upcoming triathlon and was hit and almost killed by a reckless driver. She was put in a coma for five days and her face was literally torn off. The recovery process took months and months and is still ongoing. My training was essentially non existent that fall and winter, which resulted in even more depression on top of the huge emotional black hole caused by the crash. My complete lack of fitness when the cycling season began in March made me even more depressed. To make things worse, later in the season when I should have finally been able to train hard and consistently, I found that I didn’t have the mental, physical, or emotional energy to do so. I simply couldn’t go for more than a few weeks without cracking. That’s why I switched to an easy sport. Triathlon.
As you can see, from 2014 on it would have been very hard for me to distinguish between the depression/fatigue from all those external issues, and the depression/fatigue caused by something chemically imbalanced within me. Now it seems obvious, but even a few weeks ago, before I even knew what the thyroid gland was, I chalked all those symptoms (depression, fatigue, poor sleep, etc.) to just the regular stress of training or Adelaide having been hit nine months ago. As I’ve said before, I’m sure there is quite a bit of cross over. But damn does it feel good to learn that there really is something wrong with me and it’s not just all in my head. It’s in my throat.
So to all the cyclist, triathletes, runners, and other sports enthusiasts, remember that sometimes things can actually go wrong in your body and what you’re experiencing might not be the normal side effects of hard training. We think that as athletes we’re more in tune with our bodies, but at the same time we’re deaf and blind to anything that we don’t perceive as training related. That feeling of constant fatigue might not just be from the big hours you put in the past month, and that enlarged testicle might not be caused by your worn out chamois.
*Edited January 6th, 2017:
About six months ago, long after I wrote this blog, my brother was also diagnosed with Hashimoto’s. He’s almost six years younger than me (he’s 25 years old as of this writing) and is not, nor has he been, a high level endurance athlete, though he is an elite level rock climber. But his more serious training for climbing didn’t start until he was about 23, so he hasn’t had that much time to “develop” hypothyroidism from training. His TSH was 22. That’s high, but not that high.
After he was diagnosed, I was forced to ponder whether high level endurance training and dieting were actually as large of factors for developing hypothyroidism as I thought (for someone who is also genetically predisposed to Hashis, such as myself). If his TSH is 22 at the age of 25, and mine was +150 at the age of 29, maybe that four year difference was all it took for my TSH (or his if he remained untreated) to rise to +150. Maybe it wasn’t the training at all. Maybe his TSH would have skyrocketed just like mine, whether he was doing high level endurance training or not. I guess the real test would be for him to go off medication for the next four years and get remeasured when he’s 29 and compare the numbers.
*Edited January 2021:
My TSH and other numbers remained steady through 2017 and 2018 if I remember correctly, then it all went to shit in 2019. Because of the high training load I was doing early that winter, I increased my medication from 150mg of armour thyroid to 180mg, trying to keep my TSH below or around 1.0 and my T4 within a normal range. It seems like no matter what I do, my T4 is always way too low.
I made this dose change sometime in the winter of 2018/2019 (though the negative impact took a long time to hit). The long term effect of taking this high of a dose, for month after month, ended up causing me to become hypERthyroid and my TSH plummeted to 0.015. I’d slowly developed many of the same symptoms of being hypOthyroid: fatigue, poor sleep, lack of power on the bike, and low motivation. It took longer than it should have to diagnose what was going wrong. At first I thought I might have mono, or was just depressed, or had some other hormone deficiency. But in the end, TSH testing and working with two different doctors revealed the problem. By the fall of 2019 I figured out what the problem was, but it took months for me to feel normal again (I also broke my neck in October, which is another story).
Fast forward to the end of December 2020 (last week) and I went the other way. My dose of armour thyroid (back at 150mg) was too low for the training volume I’d been doing in November and December, and I was hypOthyroid again (like usual) with a TSH approaching 4 and a T4 of 0.8. It’s a constant battle to keep my TSH around 1, which seems to be the magic number, and I’ve come to realize that I will essentially have to get tested every other month in order to ensure that I’m on the right dose. There is no doubt in my mind that hard training dose “use up” thyroid hormones. The more training you do, the higher dose of medication you need to be on. But, (and I’m hypothesizing here) the difference between doing 16 hours a week and 26 hours a week probably only requires a relatively small dose change, based on the fact that I know 150mg is too little, and 180mg is way too much.
I still think it’s possible for Hashimoto’s to compete at a high level and train their asses off, and I certainly think you should be able to expect a lot out of your body if you have this disease, but since we can’t produce thyroid hormones on our own, we have to be on top of testing and making small modifications in medication—All the time. They key may not be so much in the diet or special herbs and remedies (I am no longer eating gluten free), but in constant testing and getting an idea of where you feel and perform the best at various TSH, T3, and T4 numbers. I will continue to make updates to this blog as I learn more.
